65 year old female with community acquired pneumonia with type 1 respiratory failure with hyperglycemia (resolved) with chorea(resolved) with diabetic nephropathy with recurrent uti with iron deficiency anemia
M.Sri Nithya
Roll. No-86
This is an online E-log book to discuss our patient de-identified health data shared after taking his/ her guardians sign informed consent
Here we discuss our individual patient problems through series of inputs from available Global online community of experts with an aim to solve those patient clinical problem with collective current best evidence based inputs.
This E-log also reflects my patient centered online learning portfolio
I have been given this case to solve in an attempt to understand the topic of " Patient clinical data analysis" to develop my competancy in reading and comprehending clinical data including history, clinical finding, investigations and come up with a diagnosis and treatment plan.
CONSENT : An informed consent has been taken from the patient in the presence of the family attenders and other witnesses as well and the document has been conserved securely for future references.
Chief compliants
A 65 yr old female patient came to casualty with complaints of weakness of lt upper limb since 1 day
Cough since 4 days
HOPI
Pt was apparently asymptomatic 1 week ago then she developed generalised weakness , fell down from bed and complaints of pain in the hip
Involuntary movements of lt upper limb since 1 day to and fro
No history of speech abnormalities , weakness in the upper limb and lower limb .
No H/o memory loss and abnormal posturing .
Complaints of cough since 4 days ,it is productive scanty sputum - white to yellow ,non blood stained and non foul smelling
H/o inadequate controls of sugars from 4 months
N/H/o vomiting ,sob,loose stools ,pain abdomen
K/c/o type 2 DM since 30 yrs on infusion since 10 yrs
( Insulin - lispro 20-x-20 )
K/c/o HTN from 20 yrs on T prolomet - xl 50 mg
T. Atenolol 25 mg po/ od at 10 am
K/c/o hypothyroidism from 15 yrs on thyronorm 75 mcg
Previous treatment history
Hospitalised 1 yr ago for UTI
https://rishikoundinya.blogspot.com/2022/08/54-year-old-female-with-uncontrolled.html?m=1
H/o hysterectomy 30 yrs ago
Personal history
DIET- mixed
Appetite: Normal
Bowel and bladder movements are regular
Sleep: adequate
No allergies
Chews tobacco
Chews betel nut and betel leaf twice daily
General examination
Pt is conscious , incoherent, cooperative
Pallor present
No
Icterus
Cyanosis
Clubbing
Lymphadenopathy
Edema present B/L pitting type extending up to knee
Vitals
BP 110/70mmhg
PR 76 BPM
RR 18 cpm
Spo2 98
Grbs. 315 mg/ dl
Systemic examination
Respiratory examination
BAE +ve and normal vesicular breath sound heard
No crepts heard
CVS examination
S1S2 heard
No murmurs heard
Abdomen examination
Soft non tender
No hepatomegaly and splenomegaly
CNS examination
Higher mental functions intact
Conscious , coherent non cooperative
Speech normal
Motor system Rt. Lt
Tone. Ul. N. N
Ll. N. N
Power Ul. N. N
Ll. N. N
Reflexes B. T. S. K. A
Rt. 1+. 1+. _. 1+. _
Lt. 1+. 1+. _. 1+. _
Plantars. B/L flexors
No cerebellar and meningial signs
Provisional diagnosis
Hyperglycemia with hemiballismus K/C/o type 2 DM with HTN since 20 yrs
K/c/o hypothyroidism since 15 yrs
K/c/o CKD since 2 yrs
Diabetic nephropathy with recurrent UTI with iron deficiency anemia
Investigation
Usg abdomen
B/l grade 1-2 RPD changes with raised echogenecity
Lab investigation



X ray pa view

Ecg

Treatment
1 inj HAI 6 units /IV/ stat followed by insulin infusion 1 ml/ hr
2 IVF NS @ 75 ml/ hr
3 5 D @ 50 ml / hr
4 check grbs hrly and infusion
5 monitor vitals and inform sos
6 NBM till further orders and I/O charting
Fever chart


Dr Aashitha Sr
Dr pradeep pg 3
Dr Vinay pg 3
Dr Narsimha pg 2
Dr Ajay pg 1
Dr prachethan pg 1
Dr M. Sri Nithya (intern)
Dr. K. Rithika(intern)
ICU bed 4
New case
65/F
S
No fever spikes
Stools passed
Involuntary movements of Lt upper limb
O
Pt is c/c/ c
Bp 150/80 MMHG
Pr. 82 bpm
Grbs. 155 mg/ dl.
Temp 98.2 F
CVS S1S2 HEARD no murmurs
RS BAE + NVBS +
P/A soft nontender
CNS HMF intact
GCS. E4 V 5 M 6
A
Hyperglycemia with hemiballismus K/C/o type 2 DM with HTN since 20 yrs
K/c/o hypothyroidism since 15 yrs
K/c/o CKD since 2 yrs
Diabetic nephropathy with recurrent UTI with iron deficiency anemia
P
inj HAI ( 1 ml + 39 ml NS ) @ 2 ml / hr ( it will be increased or decreased based on grbs values)
IVF NS @ 75 ml/ hr
IVF 5 D. 50 ml/ hr
hourly grbs monitoring and monitor vitals and inform sos
T promolet Xl 50 mg po/od at 8 am
T thyronorm 75 mcg po/ od @ 7 am
T tetabenazine 12.5 mgPo/ od
On 08/2/23-
Referred to the department of ophthalmology I/v/ 0- diabetic and hypertensive retinopathy -
No diabetic retinopathy changes noted
No hypertensive retinopathy changes noted.
On 9/2/23-
Referred to the department of neurology I/v/ o generalised weakness and involuntary movements of left upper limb.
On 9/2/23-
Referred to the department of anaesthesia as patient has to undergo mri under general anaesthesia
Referred to the department of dermatology I/v/o dry, brown scaly lesions on both legs.
Diagnosed as senile xerosis.
Bacterial culture and sensitivity report-

On 13/2/23-
Referred to the department of pulmonology I/v/o- hospital acquired pneumonia with type 1 respiratory failure.
Adviced-
Cst
Syp. Ascoryl 2 tbsp po/tid
Nebulisation with mucomist BD
Chest xray PA view-

2d echo -
Treatment-
Head end elevation
Inj. Augmentin 1.2g/ iv / bd
T. Thyronorm 75 mcg po/od
T. Promet-xl 50 mg po/bd
T. Tetrabenazine 125 mg po/tid
Inj. HAI s/c tid
8am- 8 units
1pm- 8 units
8pm- 8 units
Liquid paraffin for l/a bd
T. Teczine 5 mg po / sos
Nebulisation with duolin -6th hourly budecort -12 th hourly
Inj. Lasix 40 mg iv/bd
IVF- NS@80 ml /hr
Grbs monitoring
Input and output monitoring







14/02/23
ICU-BED NO. 2
UNIT 2
Dr Aashitha(SR)
Dr Pradeep PGY3
Dr Vinay PGY3
Dr Narsimha PGY2
Dr prachethan PGY1
Dr Ajay PGY1
S
C/O COUGH WITH EXPECTORANTION DECREASED
STOOLS PASSED
NO FEVER SPIKES SINCE YESTERDAY NIGHT
O
PT IS C/C/C
TEMP-AFEBRILE
PR-78Bpm
SPO2-99% WITH 2L OF O2
BP-120/60mmhg
Grbs-
8 am -170 mg/dl
8 units hai given
1pm - 132 mg/dl given 6 units hai
O/E-
SYSTEMIC EXAMINATION -
CVS-S1, S2 +
No Murmurs
RS-BAE+, crepts + in left infrascapular ,infra axillary areas
CNS- No focal Neurological deficit
P/A - Soft ,Nontender
A-
70 yrs old Female with HOSPITAL ACQUIRED PNEUMONIA WITH TYPE 1RESPIRATORY FAILURE
WITH HYPERGLYCEMIA RESOLVED WITH CHOREA RESOLVED WITH DIABETIC NEPHROPATHY WITH REFURRENT UTI WITH IRON DEFICIENCY ANEMIA
K/C/O DM2 SINCE 30 YRS
K/C/I HYPOTHYROIDISM SINCE 15 YRS.
K/C/O CKD SINCE 2 YRS
P-
Head end elevation
Inj. Augmentin 1.2g/ iv / bd
T. Thyronorm 75 mcg po/od
T. Promet-xl 50 mg po/bd
T. Tetrabenazine 12.5 mg po/tid
Inj. HAI s/c tid
8am- 8 units
1pm- 8 units
8pm- 8 units
Liquid paraffin for l/a bd
T. Teczine 5 mg po / sos
Nebulisation with budecort -12 th hourly
Mucomist -10 th hourly
Inj. Lasix 20 mg iv/bd
IVF- NS@50 ml /hr
Grbs monitoring
Input and output monitoring
15/02/23
ICU-BED NO. 2
UNIT 2
70 yrs old Female came with c/o generalised weakness since 1 week,
Involuntary movements of left upper limb since 1 week, cought with expectoration since 1 week
S
C/O COUGH WITH EXPECTORANTION DECREASED
STOOLS PASSED YESTERDAY
NO FEVER SPIKES SINCE YESTERDAY NIGHT
O
PT IS C/C/C
TEMP-AFEBRILE
PR-78Bpm
SPO2-99% WITH 2L OF O2
BP-120/60mmhg
Grbs-
8 am -231 mg/dl
10 units hai given
O/E-
SYSTEMIC EXAMINATION -
CVS-S1, S2 PRESENT
NO MURMURS
RS-BAE+, crepts + in left infrascapular ,infra axillary areas
CNS- No focal Neurological deficit
P/A - Soft ,Nontender
Investigations -
S. Creatine-2. 8
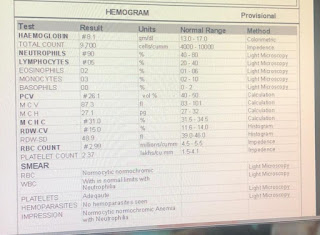
Hb-7.8
TLC -15200
Neutrophils -75
Lymphocytes -12
Pcv-24.8
Mcv-58.9
Mch- 18.5
Mchc-31. 3
Rdw-16. 6
Platelet-2. 81
Na-134
K-3.8
Cl-102
Ca2+-1.11
Blood urea-102
A-
70 yrs old Female with HOSPITAL ACQUIRED PNEUMONIA WITH TYPE 1RESPIRATORY FAILURE( resolving)
WITH HYPERGLYCEMIA( RESOLVED )WITH CHOREA (RESOLVED) WITH DIABETIC NEPHROPATHY WITH REFURRENT UTI WITH IRON DEFICIENCY ANEMIA
K/C/O DM2 SINCE 30 YRS
K/C/I HYPOTHYROIDISM SINCE 15 YRS.
K/C/O CKD SINCE 2 YRS
P-
Head end elevation
IVF- NS@50 ml /hr
Inj. Augmentin 1.2g/ iv / bd-( day 2)
Inj. HAI s/c tid
8am- 8 units
1pm- 8 units
8pm- 8 units
T. Thyronorm 75 mcg po/od
T. Promet-xl 50 mg po/bd
T. Tetrabenazine 12.5 mg po/tid
T. Teczine 5 mg po / sos
Liquid paraffin for l/a bd
Nebulisation with budecort -12 th hourly
Mucomist -10 th hourly
Grbs monitoring
Input and output monitoring

Comments
Post a Comment