GENRAL MEDICINE [E BLOGS]
CASE-11) Pulmonology (10 Marks)
1)EVOLUTION OF EVENTS OF SYMPTOMATOLOGY
1)shortness of breath which is on and off since 20 years.
2)pedal edema since 15 days up to the level of the ankle, pitting type.
3)facial puffiness since 15 days
4)drowsiness since 2 days
5)decreased urine output since 2 days
Sob
1st episode of sob 20 years ago (2001) which is sudden in onset and lasted for 1 week. It was relieved on taking medication.
For next 8 years similar episodes of sob for 1 week with no increase in severity at the same time every year in the month of january and were relieved upon medications.
12 years ago another episode of sob ,increase in severity that lasted for 20 days for which she has been hospitalised and treated
For the next years-yearly episodes -not mentioned about the severity and duration-?
Latest episode of sob 30 days ago which was initially grade 2 and then progressed to grade 4 which was not relieved on medications and now currently on intermittent bipap.
ANATOMICAL LOCALISATION OF THE PROBLEM-- IN THE REPIRATORY SYSTEM (LUNGS) AND CARIOVASCULAR SYSTEM(HEART)
PRIMARY ETIOLOGY OF THE PATIENT PROBLEM -
Acute exacerbation of COPD associated with right heart failure and bronchiectasis.
2)MECHANISM OF ACTION, INDICATION AND EFFICACY OF THE INTERVENTIONS
- HEAD END ELEVATION 30/45DEGREES - USED IN MECHANICALLY VENTILATED PEOPLE
- FOR DECREASING INCIDENCE OF ASPIRATION AND VENTILATOR ASSOCIATED PNEUMONIA. IT ALSO SHOWN TO IMPROVE OXYGENATION AND HEMODYNAMIC PERFORMANCE.
- O2 inhalation to maintain SPO2 above 92%
- Intermittent BiPAP for 2hrs TO SUPPORT VENTILATION
- Inj. AUGUMENTIN 1.2gm IV BO-Augmentin contains two drugs: amoxicillin ( beta lactam antibiotic) and clavulanic acid( beta lactamase inhibitor). This combination makes Augmentin work against more types of bacteria than antibiotics that contain amoxicillin alone.
Augmentin is effective for treating infections caused by many different types of bacteria. These include bacteria that cause:
- pneumonia
- ear infections
- sinus infections
- skin infections
- urinary tract infections.
The more common side effects of Augmentin include:
- diarrhea
- nausea
- skin rash
- vaginitis (caused by problems such as yeast infection)
- vomiting
Serious side effects
- Liver problems. Symptoms can include:
- stomach pain
- fatigue
- yellowing of your skin or the whites of your eyes
- Intestinal infection. Symptoms can include:
- severe diarrhea that doesn’t go away
- stomach pain or cramping
- nausea
- blood in your stool
- Allergic reaction. Serious allergic reactions can occur in some people who take Augmentin. This is more likely to happen in people with a penicillin allergy. Symptoms of an allergic reaction can include:
- severe skin rash
- hives
- swelling of the lips, tongue, throat
- trouble breathing
Rash
Rash occurs in about 3 percent of people who take Augmentin.
Raised, itchy, white, or red bumps that occur after the first couple doses of Augmentin may indicate an allergy to the medication.
Yeast infection
Vaginal yeast infections can sometimes occur after treatment with antibiotics, including Augmentin.
- TAB. AZITHROMYCIN 500mg OD--it belongs to macrolide group of antibiotics.


- INJ. LASIX IV BO if SBP greater than 110 mmHg--furosemide, a loop diuretic

- TAB PANTOP 40mg PO OD- Pantoprezole, a proton pump inhibitor.
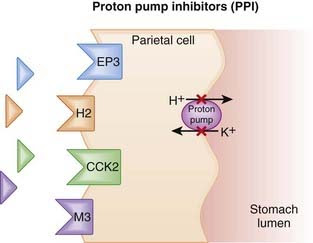
Common side effects : include headaches, diarrhea, vomiting, abdominal pain, and joint pain.[4] More serious side effects may include severe allergic reactions, a type of chronic inflammation known as atrophic gastritis, Clostridium difficile colitis, low magnesium, and vitamin B12 deficiency.[4] Use in pregnancy appears to be safe.[4] Pantoprazole is a proton pump inhibitor that decreases gastric acid secretion.[4] It works by inactivating (H+/K+)-ATPase function in the stomach.[7][4]
- INJ. HYDROCORTISONE 100 mg IV- it is steroid.

- rheumatic disorders, such as rheumatoid arthritis and ankylosing spondylitis
- eye conditions, such as severe allergic and inflammatory conditions
- stomach or intestinal disorders, such as ulcerative colitis and intestinal swelling
- collagen disorders, such as systemic lupus erythematosus
- endocrine disorders, such as thyroid inflammation
- respiratory disorders, such as Loeffler’s syndrome or inflammation of the lung due to beryllium or aspiration
- infections, such as tuberculosis, meningitis in tuberculosis, and roundworm infections
- to slow down your immune system (immunosuppression):
- skin disorders, such as pemphigus, Stevens-Johnson syndrome, exfoliative dermatitis, mycosis fungoides, severe psoriasis, or seborrheic dermatitis
- allergies. It’s used as treatment of severe conditions if other therapy doesn’t work. These include allergic rhinitis, bronchial asthma, skin reactions, serum sickness, and allergic reactions to medications.
- blood disorders, such as idiopathic thrombocytopenic purpura and secondary thrombocytopenia in adults, red blood cell anemia, autoimmune hemolytic anemia, and congenital hypoplastic anemia
- fluid retention (edema)
- cancer-related conditions, such as leukemia symptoms, lymphoma symptoms, and hypercalcemia associated with cancer
- Allergic reactions. Symptoms can include:
- skin rash
- itching
- hives
- swelling of your face, lips, or tongue
- breathing problems
- Infection. Symptoms can include:
- fever
- sore throat
- sneezing
- cough
- wounds that won’t heal
- pain when urinating
- Mental changes, such as:
- depression
- mood swings
- Stomach problems, including:
- vomiting
- severe stomach pain
- Central serous chorioretinopathy. Symptoms can include:
- distorted vision
- blind spot in your line of vision
- objects looking smaller or farther away than they really are
- Epidural lipomatosis. Symptoms can include:
- fatty deposits on your back
- back pain
- weakness or numbness in your legs or feet
- Pheochromocytoma crisis. Symptoms can include:
- high blood pressure
- rapid heartbeat
- excessive sweating
- severe headache
- tremors
- paleness in your face
- Pain in your hips, back, ribs, arms, shoulders, or legs
- High blood sugar. Symptoms can include:
- passing urine more often than usual
- increased thirst
- feeling hungrier than normal
- Feeling unusually weak or tired
- Swelling of your feet or lower legs
- Seizures
- NEB. with IPRAVENT, BUDECORT 6 hrly-

- TAB PULMOCLEAR 100 mg PO OD- It contains Acetylcysteine+Acebrophylline

- Indications: For the treatment of adult patients with chronic obstructive pulmonary disease (COPD)
- chest physiotherapy
- GRBS 6 hrly
- INJ. HAI SC ( 8 am- 2pm- 8pm)-- insulin for treating diabetes
- Temp, BP, PR, SPO2 monitoring
- I/O charting
- INJ. THIAMINE 1 amp in 100 ml of NS.- moa:- combines with ATP in liver , kidney & leucocytes produces thiamine diphosphate which acts as a coenzyme in carbohydrate metabolism in transketolation
Indication :- for low levels of thiamine. For digestive problems (alcoholics have thiamine deficiency)
(1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans) Type 2 DM - since 2 YRS
Seizures (2-3 eps) - 1month ago
Seizures -4months ago
Short term memory loss -9 days ago
Started talking - 9days ago
Started laughing -9 days ago
He was unable to lift himself off bed - since 9 days
Decreased food intake - since 9days
General body pains -1 day ago
Anatomical localisation :- brain (prefrontal cortex,hypothalamus & limbic system)
Primary etiology :- alcohol
(2) What are mechanism of action, indication and efficacy over placebo of each of the
pharmacological and non pharmacological interventions used for this patient?
Ans) RL & NS :- Electrolyte replenishment
Thiamine :- moa:- combines with ATP in liver , kidney & leucocytes produces thiamine diphosphate which acts as a coenzyme in carbohydrate metabolism in transketolation
Indication :- for low levels of thiamine. For digestive problems (alcoholics have thiamine deficiency)
Lorazepam:- moa :- lorazepam binds to benzodiazepine receptors on postsynaptic GABA-A ligand gated clorine channel neuron at several sites within the CNS. It Inhibits the effects of GABA which increases the conductance of chlorine ions into the cell
Indication :- anxiety disorfers with/ without depression symptoms
Pregabakin :- moa :- it may reduce excitatory neurotransmitter release by binding to the α2-δ protein subunit of voltage-gated calcium channels
(3) Why have neurological symptoms appeared this time, that were absent during withdrawal earlier?
What could be a possible cause for this?
Ans) Excessive drinking excites and irritates N.S
Body will be dependent on daily basis for alcohol
CNS cannot adapt without alcohol
Cessation of alcohol leads to alcohol withdrawal symptoms.
(4) What is the reason for giving thiamine in this patient?
Ans)Alcoholics have thiamine deficiency. As the patient decreased his food intake since 9days ge has been diagnosed as thiamine deficiency as thiamine is not produced in our body.
Thiamine is administered to the patient in order to keep the nervous system healthy
(5) What is the probable reason for kidney injury in this patient?
Ans) DEHYDRATION
(6). What is the probable cause for the normocytic anemia?
Ans) kidney failure - as erythropoeitin is produced in kidney which plays a key role in the production of RBCs
(7) Could chronic alcoholism have aggravated the foot ulcer formation? If yes, how and why
Ans) yes, it has aggrevated the foot ulcer formation due to anaemia caused by alcoholism
- 1) history of giddiness 7 days back. It started at around 7 am when the patient was doing his usual morning routine. He suddenly felt giddy and took rest, after which it subsided briefly.
- This was associated with 1 episode of vomiting on the same day.
- He then developed giddiness, that was sudden in onset, continuous and gradually progressive. It increased in severity upon getting up from the bed and while walking.
- Bilateral Hearing loss, aural fullness and presence of tinnitus.
- He has associated vomiting- 2-3 episodes per day, non projectile, non bilious containing food particles.
- Patient has H/o postural instability- he is unable to walk without presence of supports, swaying is present and he has tendency to fall while walking
- then pt developed slurring of speech and deviation of mouth 2 days back.
Primary etiology of the pts problem;
VERTIN 8MG TABLET compromises of Betahistine that works by enhancing the blood flow to the affected part of the ear and also by reducing the amount of fluid in the inner ear. This drug also reduces the number of attacks a person can have.
-Inj Zofer 4 mg IV/TID- it contains ondensetron, an anti emetic drug.

Tab Ecosprin 75 mg PO/OD

Tab Atorvostatin 40 mg PO/HS- to improve lipid profile

BP monitoring- 4rth hourly as he was diagnosed with denovo hypertension
Tab Clopidogrel 75 mg PO/OD

Inj Thiamine 1 AMP in 100 ml NSPO/BD
Tab MVT PO/OD-
Thiamine plays an important role in helping the body convert carbohydrates and fat into energy. It is essential for normal growth and development and helps to maintain proper functioning of the heart and the nervous and digestive systems.
For the treatment of thiamine and niacin deficiency states, Korsakov's alcoholic psychosis, Wernicke-Korsakov syndrome, delirium, and peripheral neuritis.
ADVICE ON DISCHARGE-
Tab Vertin 8 mg PO TID - 1 week
Tab Zofer 4 mg IV/TID - 1 week
Tab Ecosporin 75 mg PO/OD - 1 week
Tab Atorvostatin 40 mg PO/HS - 1 week
Tab Clopidogrel 75 mg PO/OD - 1 week
Tab MVT PO/OD - 1 week
- 3)HSTORY OF DENOVO HYPERTENSION;
- history of denovo hypertension has a huge role to play . As hypertension has a huge role in the pathogenesis of cerebrovascular accident.

Acute ischaemic strokes occur due to an occlusion of an intracranial or cervical artery with consequent deprivation of blood and oxygen to a brain territory. A few minutes after an arterial occlusion in the brain, a core ischaemic lesion is established, however a larger area at risk of hypoperfusion can be salvageable if recanalisation therapies are administered. The salvageable area or ischaemic penumbra is largely dependent on collateral blood flow and acute reductions of BP can threaten perfusion in critical areas.[25]
In the acute phase of ischaemic stroke, early initiation or resumption of antihypertensive treatment is indicated only in patients treated with recombinant tissue-type plasminogen activator or if hypertension is extreme.

10 yrs back had the episode of paralysis of both upper and lowerlimbs(rt and left)
(right and left)paresis due to hypokalemia 1year back
*Swelling over the legs(bilateral)-8 months-gradually progressing and it is present both in sitting and standing position and relieved on taking medication.
Pain along her left upper limb associated with tingling and numbness-6 days
Chestpain -since5 days
*Difficulty in breathing-5 days
Palpitations: since 5days-which are sudden in onset,more during night time and aggregated by lifting weights, speaking continuously and it is relieved by drinking more water, medication
*dyspnoea during palpitations (NYHA-CLASS-3)-since5 days.
ANATOMICAL LOCALIZATION OF THE PROBLEM;
CERVICAL VERTEBRAE AND ELECTROLYTE IMBALANCE
PRIMARY ETIOLOGY OF THE PATIENT;
CERVICAL SPONDYLOSIS AND RECURRENT HYPOKALEMIC PERALYSIS.
2)CAUSES FOR RECURRENT HYPOKALEMIA IN THIS PATIENT MAY BE DUE TO INADEQUATE INTAKE OF POTASSIUM OR DUE TO EXCESS LOSS OF POTASSIUM IN THE URINE.
OTHER CAUSES OF HYPOKALEMIA;
Causes of hypokalemia.
| Gastrointestinal tract losses | • Chronic diarrhea, including chronic laxative abuse and bowel diversion • Clay (bentonite) ingestion, which binds potassium and greatly decreases absorption • Villous adenoma of the colon, which causes massive potassium secretion (rarely) |
| Intracellular shift | • Glycogenesis during total parenteral nutrition or enteral hyperalimentation (stimulating insulin release) • Insulin administration • Stimulation of the sympathetic nervous system, particularly with beta 2-agonists (albuterol, terbutaline) • Thyrotoxicosis (occasionally) due to excessive beta-sympathetic stimulation (hypokalemic thyrotoxic periodic paralysis) • Familial periodic paralysis |
| Renal potassium losses | • Adrenal steroid excess (Cushing’s syndrome) • Primary hyperaldosteronism • Rare renin-secreting tumors • Glucocorticoid-remediable congenital adrenal hyperplasia. • Ingestion of substances such as glycyrrhizin • Bartter syndromeGitelman syndrome Liddle syndrome • Renal tubular acidosis Fanconi syndrome • Hypomagnesemia |
| Drugs | • Thiazides • Loop diuretics • Osmotic diuretics • Laxatives • Amphotericin B |
- Medications like diuretics
- Heart failure
- Hypertension
- Low BMI
- Diarrhea, cushing syndrome, and any condition that cause increase potassium loss
The ECG in hypokalemia may appear normal or may have only subtle findings immediately before clinically significant dysrhythmias. ECG findings may include the following:
- Ventricular dysrhythmia
- Prolongation of QT interval [53]
- ST-segment depression
- T-wave flattening
- Appearance of U waves
- Ventricular arrhythmias (eg, premature ventricular contractions [PVCs], torsade de pointes, ventricular fibrillation) [54]
- Atrial arrhythmias (eg, premature atrial contractions [PACs], atrial fibrillation)
The symptoms of hypokalemia are nonspecific and predominantly are related to muscular or cardiac function.
-Weakness and fatigue are the most common complaints.
The muscular weakness that occurs with hypokalemia can manifest in protean ways (eg, dyspnea, constipation or abdominal distention, exercise intolerance).
-Rarely, muscle weakness progresses to frank paralysis. With severe hypokalemia or total body potassium deficits, muscle cramps and pain can occur with rhabdomyolysis.
Occasionally, a patient may complain of worsening diabetes control or polyuria due to a recent onset of hyperglycemia or nephrogenic diabetes insipidus.
-Patients also may complain of palpitations.
-Psychological symptoms may include psychosis, delirium, hallucinations, and depression.
The brain consists of nerve cells that communicate with each other through electrical activity. A seizure occurs when one or more parts of the brain has a burst of abnormal electrical signals that interrupt normal brain signals. Anything that interrupts the normal connections between nerve cells in the brain can cause a seizure. This includes a high fever, high or low blood sugar, alcohol or drug withdrawal, or a brain concussion. But when a person has 2 or more seizures with no known cause, this is diagnosed as epilepsy.
There are different types of seizures. The type of seizure depends on which part and how much of the brain is affected and what happens during the seizure. The 2 main categories of epileptic seizures are
1) focal (partial) seizure and
2)generalized seizure.
1)Focal (partial) seizures
Focal seizures take place when abnormal electrical brain function occurs in one or more areas of one side of the brain. Before a focal seizure, you may have an aura, or signs that a seizure is about to occur. This is more common with a complex focal seizure. The most common aura involves feelings, such as deja vu, impending doom, fear, or euphoria. Or you may have visual changes, hearing abnormalities, or changes in your sense of smell. The 2 types of focal seizures include:
Simple focal seizure
The symptoms depend on which area of the brain is affected. If the abnormal electrical brain function is in the part of the brain involved with vision (occipital lobe), your sight may be altered. More often, muscles are affected. The seizure activity is limited to an isolated muscle group. For example, it may only include the fingers, or larger muscles in the arms and legs. You may also have sweating, nausea, or become pale. You don’t lose consciousness in this type of seizure.
Complex focal seizure
This type of seizure often occurs in the area of the brain that controls emotion and memory function (temporal lobe). You will likely lose consciousness. This may not mean you pass out. You may just stop being aware of what's going on around you. You may look awake, but have a variety of unusual behaviors. These may range from gagging, lip smacking, running, screaming, crying, or laughing. You may be tired or sleepy after the seizure. This is called the postictal period.
2)Generalized seizure
A generalized seizure occurs in both sides of the brain. You will lose consciousness and be tired after the seizure (postictal state). Types of generalized seizures include:
Absence seizure
This is also called petit mal seizure. This seizure causes a brief changed state of consciousness and staring. You will likely maintain your posture. Your mouth or face may twitch or your eyes may blink rapidly. The seizure usually lasts no longer than 30 seconds. When the seizure is over, you may not recall what just occurred. You may go on with your activities as though nothing happened. These seizures may occur several times a day.
Atonic seizure
This is also called a drop attack. With an atonic seizure, you have a sudden loss of muscle tone and may fall from a standing position or suddenly drop your head. During the seizure, you will be limp and unresponsive.
Generalized tonic-clonic seizure (GTC)
This is also called grand mal seizure. The classic form of this kind of seizure has 5 distinct phases. Your body, arms, and legs will flex (contract), extend (straighten out), and tremor (shake). This is followed by contraction and relaxation of the muscles (clonic period) and the postictal period. During the postictal period, you may be sleepy. You may have problems with vision or speech, and may have a bad headache, fatigue, or body aches. Not all of these phases occur in everyone with this type of seizure.
Myoclonic seizure
This type of seizure causes quick movements or sudden jerking of a group of muscles. These seizures tend to occur in clusters. This means that they may occur several times a day, or for several days in a row.
-YES,there is relation between the occurance of seizures and brain stroke.
RELATION BETWEEN BRAINSTROKE AND SEIZURE;

1) REASON FOR THIS PATIENT TO DEVELO[P ATAXIA ;
Ataxia describes a lack of muscle control or coordination of voluntary movements, such as walking or picking up objects. A sign of an underlying condition, ataxia can affect various movements and create difficulties with speech, eye movement and swallowing.
This patient developed persistent ataxia during past one year due to stroke in frontal, parietal and temporal lobes which are resulted due to head trauma that were left untreated.
other causes of ataxia;
Damage, degeneration or loss of nerve cells in the part of your brain that controls muscle coordination (cerebellum), results in ataxia. Cerebellum comprises two portions of folded tissue situated at the base of your brain near your brainstem. This area of the brain helps with balance as well as eye movements, swallowing and speech.
Diseases that damage the spinal cord and peripheral nerves that connect your cerebellum to your muscles also can cause ataxia. Ataxia causes include:
- Head trauma. Damage to your brain or spinal cord from a blow to your head, such as might occur in a car accident, can cause acute cerebellar ataxia, which comes on suddenly.
- Stroke. Either a blockage or bleeding in the brain can cause ataxia. When the blood supply to a part of your brain is interrupted or severely reduced, depriving brain tissue of oxygen and nutrients, brain cells die.
- Cerebral palsy. This is a general term for a group of disorders caused by damage to a child's brain during early development — before, during or shortly after birth — that affects the child's ability to coordinate body movements.
- Autoimmune diseases. Multiple sclerosis, sarcoidosis, celiac disease and other autoimmune conditions can cause ataxia.
- Infections. Ataxia can be an uncommon complication of chickenpox and other viral infections such as HIV and Lyme disease. It might appear in the healing stages of the infection and last for days or weeks. Normally, the ataxia resolves over time.
- Paraneoplastic syndromes. These are rare, degenerative disorders triggered by your immune system's response to a cancerous tumor (neoplasm), most commonly from lung, ovarian, breast or lymphatic cancer. Ataxia can appear months or years before the cancer is diagnosed.
- Abnormalities in the brain. An infected area (abscess) in the brain may cause ataxia. A growth on the brain, cancerous (malignant) or noncancerous (benign), can damage the cerebellum.
Toxic reaction. Ataxia is a potential side effect of certain medications, especially barbiturates, such as phenobarbital; sedatives, such as benzodiazepines; antiepileptic drugs, such as phenytoin; and some types of chemotherapy. Vitamin B-6 toxicity also may cause ataxia. These causes are important to identify because the effects are often reversible.
Also, some medications you take can cause problems as you age, so you might need to reduce your dose or discontinue the medication.
Alcohol and drug intoxication; heavy metal poisoning, such as from lead or mercury; and solvent poisoning, such as from paint thinner, also can cause ataxia.
- Vitamin E, vitamin B-12 or thiamine deficiency. Not getting enough of these nutrients, because of the inability to absorb enough, alcohol misuse or other reasons, can lead to ataxia.
- Thyroid problems. Hypothyroidism and hypoparathyroidism can cause ataxia.
- COVID-19 infection. This infection may cause ataxia, most commonly in very severe cases.
For some adults who develop sporadic ataxia, no specific cause can be found. Sporadic ataxia can take a number of forms, including multiple system atrophy, a progressive, degenerative disorder.
Hereditary ataxias
Some types of ataxia and some conditions that cause ataxia are hereditary. If you have one of these conditions, you were born with a defect in a certain gene that makes abnormal proteins.
The abnormal proteins hamper the function of nerve cells, primarily in your cerebellum and spinal cord, and cause them to degenerate. As the disease progresses, coordination problems worsen.
You can inherit a genetic ataxia from either a dominant gene from one parent (autosomal dominant disorder) or a recessive gene from each parent (autosomal recessive disorder). In the latter case, it's possible neither parent has the disorder (silent mutation), so there might be no obvious family history.
Different gene defects cause different types of ataxia, most of which are progressive. Each type causes poor coordination, but each has specific signs and symptoms.
Autosomal dominant ataxias
These include:
- Spinocerebellar ataxias. Researchers have identified more than 40 autosomal dominant ataxia genes, and the number continues to grow. Cerebellar ataxia and cerebellar degeneration are common to all types, but other signs and symptoms, as well as age of onset, differ depending on the specific gene mutation.
Episodic ataxia (EA). There are eight recognized types of ataxia that are episodic rather than progressive — EA1 through EA7, plus late-onset episodic ataxia. EA1 and EA2 are the most common. EA1 involves brief ataxic episodes that may last seconds or minutes. The episodes are triggered by stress, being startled or sudden movement, and often are associated with muscle twitching.
EA2 involves longer episodes, usually lasting from 30 minutes to six hours, which also are triggered by stress. You might have dizziness (vertigo), fatigue and muscle weakness during your episodes. In some cases, symptoms resolve in later life.
Episodic ataxia doesn't shorten life span, and symptoms might respond to medication.
Autosomal recessive ataxias
These include:
Friedreich's ataxia. This common hereditary ataxia involves damage to your cerebellum, spinal cord and peripheral nerves. Peripheral nerves carry signals from your brain and spinal cord to your muscles. In most cases, signs and symptoms appear well before age 25.
The rate of disease progression varies. The first indication generally is difficulty walking (gait ataxia). The condition typically progresses to the arms and trunk. Muscles weaken and waste away over time, causing deformities, particularly in your feet, lower legs and hands.
Other signs and symptoms that might develop as the disease progresses include slow, slurred speech (dysarthria); fatigue; rapid, involuntary eye movements (nystagmus); spinal curvature (scoliosis); hearing loss; and heart disease, including heart enlargement (cardiomyopathy) and heart failure. Early treatment of heart problems can improve quality of life and survival.
Ataxia-telangiectasia. This rare, progressive childhood disease causes degeneration in the brain and other body systems. The disease also causes immune system breakdown (immunodeficiency disease), which increases susceptibility to other diseases, including infections and tumors. It affects various organs.
Telangiectasia is the formation of tiny red "spider" veins that might appear in the corners of your child's eyes or on the ears and cheeks. Delayed motor skill development, poor balance and slurred speech are typically the first indications of the disease. Recurrent sinus and respiratory infections are common.
Children with ataxia-telangiectasia are at high risk of developing cancer, particularly leukemia or lymphoma. Most people with the disease need a wheelchair by their teens and die before age 30, usually of cancer or lung (pulmonary) disease.
- Congenital cerebellar ataxia. This type of ataxia results from damage to the cerebellum that's present at birth.
- Wilson's disease. People with this condition accumulate copper in their brains, livers and other organs, which can cause neurological problems, including ataxia. Early identification of this disorder can lead to treatment that will slow progression.
- Blood clotting, or coagulation, an important physiological process that ensures the integrity of the vascular system, involves the platelets, or thrombocytes,4 as well as several proteins dissolved in the plasma.
- When a blood vessel is injured, platelets are attracted to the site of the injury, where they aggregate to form a temporary plug.
- The platelets secrete several proteins (i.e., clotting factors) that—together with other proteins either secreted by surrounding tissue cells or present in the blood—initiate a chain of events that results in the formation of fibrin
- Fibrin is a stringy protein that forms a tight mesh in the injured vessel; blood cells become trapped in this mesh, thereby plugging the wound.
- Fibrin clots, in turn, can be dissolved by a process that helps prevent the development of thrombosis (i.e., fibrinolysis).
- Alcohol can interfere with these processes at several levels, causing, for example, abnormally low platelet numbers in the blood (i.e., thrombocytopenia), impaired platelet function (i.e., thrombocytopathy), and diminished fibrinolysis. These effects can have serious medical consequences, such as an increased risk for strokes.
- In addition to differences in the quantity of alcohol consumed, inherited or acquired variations in an individual drinker’s biochemistry may account for these differences in susceptibility.
- Thrombocytopathy Alcohol affects not only platelet production but also platelet function. Thus, patients who consume excessive amounts of alcohol can exhibit a wide spectrum of platelet abnormalities when admitted to a hospital.
- These abnormalities include impaired platelet aggregation, decreased secretion or activity of platelet-derived proteins involved in blood clotting, and prolongation of bleeding in the absence of thrombocytopenia.
- Because alcohol impairs the function of the normal blood-clotting system, it also can adversely interact with over-the-counter and prescription medications that prolong bleeding or prevent coagulation.
- For example, alcohol can potentiate the prolongation of bleeding time caused by aspirin and other nonsteroidal anti-inflammatory drugs (NSAID’s) (e.g., ibuprofen or indomethacin), particularly when alcohol ingestion equivalent to about four drinks occurs simultaneously with or following ingestion of normal doses of these medications.
- As a result, the concomitant use of alcohol and aspirin or NSAID’s greatly increases the patient’s risk for gastrointestinal bleeding. Similarly, alcohol can enhance aspirin-induced fecal blood loss.
- During a hemorrhagic stroke, the blood flow to a brain area is impaired due to a ruptured blood vessel that results in bleeding in the brain.
- If the blood flow is interrupted because a blood vessel is blocked by a blood clot, the condition is called an ischemic stroke.
- Alcohol conceivably can contribute to both conditions by interfering with the normal coagulation system and by reducing fibrinolysis, respectively.
- For example, researchers have suggested that acetaldehyde interacts with some proteins of the blood-clotting system and thus induces abnormal coagulation. In addition to these direct effects on the blood components, alcohol may increase the risk of a stroke indirectly by altering the drinker’s blood pressure; heart rate; tone of the heart muscles; and “thickness,” or viscosity, of the blood .
1)yes, the pt history of cva has major role in the development of the disease. there is dislocation of the shoulder, mandible and zygomatic in that accident. there might be damage to the middle cerebral artery that may went unnoticed initially.
Areas supplied by the middle cerebral artery include: The bulk of the lateral surface of the hemisphere; except for the superior inch of the frontal and parietal lobe (anterior cerebral artery), and the inferior part of the temporal lobe.
and now in the CT we can see the altered signal intensity in the areas involving the left caudate nucleus, lentiform nucleus ,left frontal and left temporal areas.
2) signs of cva in this pt are;
1. WEAKNESS OF RIGHT UPPERLIMB AND LOWER LIMB SINCE ONE DAY.
2.DEVIATION OF MOUTH TOWARDS LEFT SINCE ONE DAY.
. Since the body is affected on the opposite side of where the stroke occurs in the brain, having one-sided facial drooping or weakness on one side of the body is common. The most frequently observed indicators in an emergency setting are the following:
Facial drooping, typically on one side of the face
Vision loss in one eye, or blurred or double vision
Weakness or numbness on one side of the body
Lack of movement or sensation on one side of the body
Loss of balance
Slurred speech or absence of speech
Altered level of consciousness
3) drug rationale in cva;
- 1.Injection Mannitol 100ml/IV/TD -it is an osmotic diuretic. it is used to decrease the cerebral edema. MOA--

- 2.TAB Ecospirin 75 mg po/OD aspirin, irreversibly inactivates platelet cyclooxygenase, which is responsible for prostaglandin and thromboxane synthesis..Initial manifestations of acute cerebral ischemia, such as ischemic stroke and transient ischemic attack (TIA), are often followed by recurrent vascular events, including recurrent stroke.2 To reduce this burden, antiplatelet therapy is a key component of the management of noncardioembolic ischem3.TAB ATORVAS 40mg po/HS
 4.BP/PR/TEMP/SP02 MONITORING (4th hourly)- vitals should monitored regularly5.RT FEEDS-100ml milk with protein powder(2nd hourly)Ryle'sTube feeding is given to the patients who are in an unconscious state, under low cranial nerve palsies, or incapable of mouth feeding due to some disease.The most common conditions wanting RT Feed as a necessity include:
4.BP/PR/TEMP/SP02 MONITORING (4th hourly)- vitals should monitored regularly5.RT FEEDS-100ml milk with protein powder(2nd hourly)Ryle'sTube feeding is given to the patients who are in an unconscious state, under low cranial nerve palsies, or incapable of mouth feeding due to some disease.The most common conditions wanting RT Feed as a necessity include:– Prematurity births,
– Failure to thrive or even extreme malnutrition cases,
– Several neuromuscular and neurologic disorders,
– Severe inability to swallow food, etc.
- In particular, aspirin irreversibly blocks production of thromboxane A2.
- Thromboxane A2 is a potent platelet activator and pro-aggregant; hence by blocking thromboxane A2 synthesis, ASA is able to achieve an antiplatelet effectic stroke and TIA.
- cervical myelopathy is a common degenerative condition caused by compression on the spinal cord that is characterized by clumsiness in hands and gait imbalance.
- treatment is typically operative as the condition is progressive.
- Pathophysiology
- etiology
- degenerative cervical spondylosis (CSM)

- most common cause of cervical myelopathy
- compression usually caused by anterior degenerative changes (osteophytes, disc osteophyte complex)
- degenerative spondylolisthesis and hypertrophy of ligamentum flavum may contribute
- congenital stenosis
- symptoms usually begin when congenital narrowing combined with spondylotic degenerative changes in older patients
- OPLL
- tumor
- epidural abscess
- trauma
- cervical kyphosis
- neurologic injury
- mechanism of injury can be
- direct cord compression
- ischemic injury secondary to compression of anterior spinal artery
- Associated conditions
- lumbar spinal stenosis

- tandem stenosis occurs in lumbar and cervical spine in ~20% of patients.
- CLASSIFICATION;stop,
Nurick Classification Grade 0 Root symptoms only or normal Grade 1 Signs of cord compression; normal gait Grade 2 Gait difficulties but fully employed Grade 3 Gait difficulties prevent employment, walks unassisted Grade 4 Unable to walk without assistance Grade 5 Wheelchair or bedbound Based on gait and ambulatory function 
Ranawat Classification Class I Pain, no neurologic deficit Class II Subjective weakness, hyperreflexia, dyssthesias Class IIIA Objective weakness, long tract signs, ambulatory Class IIIB Objective weakness, long tract signs, non-ambulatory Japanese Orthopaedic Association Classification - A point scoring system (17 total) based on function in the following categories

- upper extremity motor function
- lower extremity motor function
- sensory function
- bladder function
Usually a significant improvement at 1-year po even in cases of severe myelopathy. - A point scoring system (17 total) based on function in the following categories
- 2)FINGER ESCAPE SIGN;
- when patient holds fingers extended and adducted, the small finger spontaneously abducts due to weakness of intrinsic muscle.
- 3)HOFFMAN'S REFLEX;
- Snapping patients distal phalanx of middle finger leads to spontaneous flexion of other fingers.
- Most common physical exam finding.

- 6) Infectious Disease (HI virus, Mycobacteria, Gastroenterology, Pulmonology) 10 MarksA) Link to patient details:Questions:1.Which clinical history and physical findings are characteristic of tracheo esophageal fistula?2) What are the chances of this patient developing immune reconstitution inflammatory syndrome? Can we prevent it?
1)CLINICAL HISTORY AND PHYSICAL FINDINGS OF TRACHEOESOPHAGEAL FISTULA ARE;
CLINICAL HISTORY;
COUGH AND DIFFICULTY IN SWALLOWING SINCE 2 MONTHS INITIALLY WITH SOLIDS SLOWLY PROGRESSED TO LIQUIDS.
WHEEZE IN B/L MAMMARY AREAS
LARYNGEAL CREPITUS -POSITIVE.
BARIUM STUDY SHOWS- BARIUM PRESENT IN THE BRONCHIAL TREE THROUGH FISTULA.
ALSO CRCT HAS SHOWN THAT- THERE IS FISTULOUS COMMUNICATIONN BETWEEN LEFT MAIN BRONCHUS AND MID THORACIC ESOPHAGUS FEW CM BELOW THE CARINA.
- OTHER CAUSES MIGHT BE;
SHE IS RVD POSITIVE -IN THESE PATIENTS OEOPHAGEAL CANDIDIASIS MIGHT BE THE CAUSE FOR DIFFICULTY IN SWALLOWING.
AS SHE IS TB POSITIVE - ANY ULCERS IN THE ESOPHAGOUS AND ENLARGED LYMPHNODES THAT COMPRESS THE ESOPHAGOUS MIGHT BE THE CAUSE.
2)IMMUNE RECONSTITUTION INFLAMMATORY SYNDROME;
A paradoxical clinical worsening of a known condition or the appearance of a new condition after initiating antiretroviral therapy (ART) therapy in HIV-infected patients resulting from restored immunity to specific infectious or non-infectious antigens is defined as immune reconstitution inflammatory syndrome (IRIS).
Because clinical deterioration occurs during immune recovery, this phenomenon has been described as immune restoration disease (IRD), immune reconstitution syndrome (IRS), and paradoxical reactions.
Etiology of immune reconstitution inflammatory syndrome

OTHER MECHANISMS;
The mechanism receiving the most attention involves the theory that the syndrome is precipitated by the degree of immune restoration following ART.
An alternative immunological mechanism may involve qualitative changes in lymphocyte function or lymphocyte phenotypic expression.
For instance, following ART an increase in memory CD4+ cell types is observed possibly as a result of redistribution from peripheral lymphoid tissue.
This CD4+ phenotype is primed to recognize previous antigenic stimuli, and thus may be responsible for manifestations of IRIS seen soon after ART initiation.
After this redistribution, naïve T cells increase and are thought to be responsible for the later quantitative increase in CD4+ cell counts.[4]
Thus IRIS may be due to a combination of both quantitative restoration of immunity as well as qualitative function and phenotypic expression observed soon after the initiation of ART.
The third purported pathogenic mechanism for IRIS involves host genetic susceptibility to an exuberant immune response to the infectious or noninfectious antigenic stimulus upon immune restoration. Although evidence is limited, carriage of specific HLA alleles suggests associations with the development of IRIS and specific pathogens.
Diagnostic Criteria for IRIS
French et al., have laid down criteria so as to aid the diagnosis.[6] These are:
Major criteria
Atypical presentation of “opportunistic infections (OI) or tumors” in patients responding to antiretroviral therapy.
Decrease in plasma HIV RNA level by at least 1 log10copies/mL.
Minor criteria
Increased blood CD4+ T-cell count after HAART.
Increase in immune response specific to the relevant pathogen, e.g. DTH response to mycobacterial antigens.
Spontaneous resolution of disease without specific antimicrobial therapy or tumor chemotherapy with continuation of antiretroviral therapy.
LIVER ABSCESS
ALA almost always occurs in males with a history of drinking indigenously brewed alcohol beverages in a poor socioeconomic background.
As the primary contributory factor is the male gender, we need to explore whether this gender preponderance is purely due to alcohol-related factors or whether it is due to other factors including the level of immunity of the host.
How amoeba gets into the beverage is not well understood. Most likely this is due to the unhygienic practices commonly seen at the drinking taverns or cottages in many tropical countries. The important finding observed in most of the studies is that majority of ALA patients are from a poor socioeconomic background and are manual laborers [10, 6, 11]. Poor hygiene has been associated with increased risk of amoebic liver abscesses and is directly proportionate to disease progression and extent of liver injury [14].
Parasite cysts are transmitted through contaminated food and water, making the incidence of disease high in areas of poor sanitation.
Good hygienic practices cannot be expected at these places as the majority of subjects are male farmers from lower- and middle-class backgrounds in one study [15] and 68% belonged to low socioeconomic group in another study [11]. The prevalence of asymptomatic intestinal amoebiasis is also common in these regions, although the prevalence rate varies with the methods used for screening. It is high when microscopic examination method is employed and low with the use of new molecular techniques [16].
It can be assumed that the regular visitors to these drinking places could be the source of pathogen by unhygienic practices including open air defecation, poor hand washing practices, unwashed utensils at these taverns, and the consumption of unboiled drinking water. Indeed, some studies have documented the prevalence of vectors of amoebiasis, including flies and cockroaches at these places
2)ETIOPATHOGENESIS OF LIVER ABSCESS IN CHRONIC ALCOHOLIC PATIENTS;
It is unknown why most amoebic liver abscess (ALA) cases occur in alcohol drinkers. In experimental studies, the presence of 'iron' potentiates the in-vitro growth of Entamoeba histolytica (E. histolytica), and is also known to increase its in-vivo invasiveness in animal infections. Chronic alcoholism increases the hepatic iron deposition.
We hypothesized that ALA occurs more commonly in livers with a high iron load as in alcoholics. To test this hypothesis we compared the levels of iron between ALA and non-ALA cases belonging to alcoholic and non-alcoholic groups. Out of a total of 48 ALA cases, 34 (70%) were alcoholics and 14 (30%) were non-alcoholics. After applying exclusion criteria, serum iron and liver iron stores were quantified in 20 ALA cases (10 alcoholic and 10 non-alcoholics) and compared with 20 non-ALA cases (10 alcoholics and 10 non-alcoholics). All patients of ALA had serum iron values within the normal range but higher than non-ALA cases. In the liver tissue, most patients with ALA had higher (grade II or III) iron deposition, than non-ALA cases (mostly grade I). Thus, patients with ALA, with or without alcohol indulgence, had higher iron levels when compared to the non-ALA cases. It appears that the higher incidence of ALA in alcoholic livers is possibly due to their higher iron content.
3)LIVER ABSCESS IS MOST COMMON IN THE RIGHT LOBE THAN IN THE LEFT LOBE;
Indications for percutaneous drainage are broad: essentially any abnormal fluid collection in the patient which can be accessible. Examples include:
- complicated diverticular abscess
- Crohn's disease related abscess
- complicated appendicitis with appendicular abscess
- tubo-ovarian abscess
- post-surgical fluid collections
- hepatic abscess (e.g. amoebic or post-operative)
- renal abscess or retroperitoneal abscess
- splenic abscess
Contraindications
The only common contraindications are:
- biopsy target is not accessible
- patient has a bleeding diathesis

1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
- Empirical therapy for presumed fungal infection in febrile, neutropenic patients.
- Treatment of Cryptococcal Meningitis in HIV-infected patients
- Treatment of patients with Aspergillus species, Candida species and/or Cryptococcus species infections (see above for the treatment of Cryptococcal Meningitis) refractory to amphotericin B deoxycholate, or in patients where renal impairment or unacceptable toxicity precludes the use of amphotericin B deoxycholate.
- Treatment of visceral leishmaniasis. In immunocompromised patients with visceral leishmaniasis treated with , relapse rates were high following initial clearance of parasites

Common side effects of include:
- fever,
- shaking,
- chills,
- flushing (warmth, redness, or tingly feeling),
- loss of appetite,
- dizziness,
- nausea,
- vomiting,
- stomach pain,
- diarrhea,
- headache,
- shortness of breath,
- fast breathing 1 to 2 hours after the infusion is started,
- sleep problems (insomnia), or
- skin rash.
SERIOUS SIDE EFFECTCS;
- swelling or pain at injection site,
- muscle or joint pain,
- unusual tiredness,
- weakness,
- muscle cramping,
- changes in the amount of urine,
- painful urination,
- numbness or tingling of arms or legs,
- vision changes,
- hearing changes (e.g., ringing in the ears),
- dark urine,
- severe stomach or abdominal pain,
- yellowing eyes or skin,
- swelling ankles or feet,
- fast/slow/irregular heartbeat,
- cold sweats,
- blue lips,
- easy bruising or bleeding,
- other signs of infection (e.g., fever, persistent sore throat),
- mental/mood changes,
- seizures,
- black stools, or
- vomit that looks like coffee grounds.
Managing diabetic ketoacidosis (DKA) in an intensive care unit during the first 24-48 hours always is advisable. When treating patients with DKA, the following points must be considered and closely monitored:
Correction of fluid loss with intravenous fluids
Correction of hyperglycemia with insulin
Correction of electrolyte disturbances, particularly potassium loss
Correction of acid-base balance
Treatment of concurrent infection.
Mucormycosis (sometimes called zygomycosis) is a serious but rare fungal infection caused by a group of molds called mucormycetes. These fungi live throughout the environment, particularly in soil and in decaying organic matter, such as leaves, compost piles, or rotten wood. 1
People get mucormycosis by coming in contact with the fungal spores in the environment. For example, the lung or sinus forms of the infection can occur after someone breathes in spores. These forms of mucormycosis usually occur in people who have health problems or take medicines that lower the body’s ability to fight germs and sickness. 3,6 Mucormycosis can also develop on the skin after the fungus enters the skin through a cut, scrape, burn, or other type of skin trauma.
Mucormycosis is rare, but it’s more common among people who have health problems or take medicines that lower the body’s ability to fight germs and sickness. Certain groups of people are more likely to get mucormycosis, 1–3 including people with:
- Diabetes, especially with diabetic ketoacidosis
- Cancer
- Organ transplant
- Stem cell transplant
- Neutropenia [PDF – 2 pages] (low number of white blood cells)
- Long-term corticosteroid use
- Injection drug use
- Too much iron in the body (iron overload or hemochromatosis)
- Skin injury due to surgery, burns, or wounds
- Prematurity and low birthweight (for neonatal gastrointestinal mucormycosis)
Types of mucormycosis
- Rhinocerebral (sinus and brain) mucormycosis is an infection in the sinuses that can spread to the brain. This form of mucormycosis is most common in people with uncontrolled diabetes and in people who have had a kidney transplant. 7-8
- Pulmonary (lung) mucormycosis is the most common type of mucormycosis in people with cancer and in people who have had an organ transplant or a stem cell transplant.
- Gastrointestinal mucormycosis is more common among young children than adults, especially premature and low birth weight infants less than 1 month of age, who have had antibiotics, surgery, or medications that lower the body’s ability to fight germs and sickness. 9-10
- Cutaneous (skin) mucormycosis: occurs after the fungi enter the body through a break in the skin (for example, after surgery, a burn, or other type of skin trauma). This is the most common form of mucormycosis among people who do not have weakened immune systems.
- Disseminated mucormycosis occurs when the infection spreads through the bloodstream to affect another part of the body. The infection most commonly affects the brain, but also can affect other organs such as the spleen, heart, and skin.
Types of fungi that most commonly cause mucormycosis
Examples are: Rhizopus species, Mucor species, Rhizomucor species, Syncephalastrum species, Cunninghamella bertholletiae, Apophysomyces species, and Lichtheimia (formerly Absidia) species.
TREATMENT;
Mucormycosis is a serious infection and needs to be treated with prescription antifungal medicine, usually amphotericin B, posaconazole, or isavuconazole. These medicines are given through a vein (amphotericin B, posaconazole, isavuconazole) or by mouth (posaconazole, isavuconazole). Other medicines, including fluconazole, voriconazole, and echinocandins, do not work against fungi that cause mucormycosis. Often, mucormycosis requires surgery to cut away the infected tissue.
|
|
MILD |
|
|
OUTCOME |
MODERATE |
|
|
|
|
SEVERE |
|
|
|
|
|
|
S.NO |
|
RR AND SPO2 LEVELS |
CTSI SCORE |
|
|
RR and SPO2 LEVELS |
CTSI SCORE |
CHANGE IN SEVERITY |
OUTCOME |
|
RR and SPO2 LEVELS |
CTSI SCORE |
DECREASE IN
SEVERITY(SPO2 LEVELS) |
SEQUALE OF DEATH |
OUTCOME |
|
1 |
https://gsuhithagnaneswar. |
RR:22 cyc/min Spo2:98% with room air |
|
RESOLVING |
https://nikhilasampathkumar. |
At the time of admission: RR: 22 cyc/min Spo2: 93% on room air 96% with 15 litres of o2. |
16/25 |
|
RESOLVING |
https://143vibhahegde. |
ADMISSION: RR: 34cyc/min Spo2:75% on 16L of o2 |
23/25 |
|
ARDS AND AKI |
DEATH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
https://vidya36.blogspot.com/2021/05/a-45-year-old-female-with-viral.html |
RR:24 cyc/min SPO2: 8O -85with room
air
95% with 15 lit of O2
UPDATE: RR- 22/min Spo2 : 93with room
air , 95 with 5lit of O2 |
6/25 |
RESOLVING |
https://nehapradeep99. |
At the time of admission- RR:? |
|
On 2nd of admission there
is INCREASE IN SEVERITY: Spo2: 99% with 10 L of o2. On 8th day of
admission: Spo2 : 87% with 15 L of o2. DEcREASED SEVERITY from 9th
day of admission. Spo2: 96% on 5L of o2. On 12 th day Spo2: 97% on 2L of o2. |
RESOLVING |
https://anuragreddy72. |
AT ADMISSION: Spo2: 20% on room air and was
unconscious. |
|
Patient was sent to higher covid
centres and was put on mechanical ventilation for 3 days. The patient is now doing fine. |
|
RESOLVING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
https://vaishnavimaguluri138. |
On 14-5-21 RR-? SPO2: 87% with room air. On 15-5-21 Sp O2 - 99% on 15
litres of oxygen.
On 16-5-21 Spo2: 98% with 10
litres of o2.
On 17-5-21 Spo2: 96% with 2 litres of o2. On 18-5-21 Spo2: 98% with 4 litres of o2. On 19-5-21 Spo2: 95% on room air. |
6/25 |
RESOLVING |
https://drsaranyaroshni. |
AT THE TIME OF ADMISSION; RR: 22 cyc/min Spo2:85% on room air. On 2nd day of
admission: Spo2:90% on 15 L of o2. DECREASE IN SEVERITY On 16-5-21 Spo2: 95% on 6L of o2. |
12/25 |
|
RESOLVING |
https://vijaykumarkasturi. |
At admission: RR:26 cyc/min Spo2:77% on room air |
17/25 |
On 1st day of admission Spo2:92% with 15L of o2. INCREASED SEVERITY from then. |
LIVER AND RENAL COMPLICATIONS |
DEATH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
https://meesumabbas82. |
RR:? Spo2: 99% on room air. |
|
RESOLVING |
https://bhavaniv.blogspot.com/ |
AT THE TIME OF ADMISSION- RR: 14 cyc/min Spo2:95% on room air. |
|
INCREASE IN SEVERITY: On 14-5-21 Spo2:85% on room air 98% on 10L of o2. DECREASE IN SEVERITY; ON 17-5-21 SPO2:96% WITH 2 L of o2. On 19-5-21 95% on room air. |
RESOLVING |
https://vignatha45.blogspot. |
AT ADMISSION: RR:40cyc/min Spo2:88% on 16L of o2. |
|
|
|
RESOLVING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
https://rishithareddy30. |
At the time of admission; RR: 16 cyc/min Spo2:97% on room air |
|
Increased in severity; On 14-5-21: RR:30 cyc/min Spo2:97% with -? Of o2. |
RESOLVING |
https://jahnavichatla. |
AT ADMISSION: RR:38cyc/min Spo2: 85% on room air 91% on 12L of o2. |
21/25 |
On 22-4-21 Spo2: 95% on 10L of o2. He was shifted to another hospital and from
then there is decrease in severity. |
|
RESOLVING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
https://93deepanandikonda. |
At the time of diagnosis; RR: 24 cyc/min Spo2:82% on room air. |
16/25 |
INCREASED IN SEVERITY: ON 18-5-21 SPO2:85% ON 15L O2. ON 19-5-21 95% WITH BiPAP. ON 24-5-21 93% ON 15L OF O2 |
RESOLVING |
https://sudhamshireddy. |
At admission: RR:18cyc/min Spo2: 93% on room air. |
|
INCREASE IN SEVERITY: ON 6-5-21; Spo2: 89% on room air 95% on4L of o2 On 8-5-21 Spo2: 56% on room air |
ARDS |
DEATH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
https://meghanaraomuddada. |
AT THE TIME OF ADMISSION: RR: 30 cyc/min Spo2: 86% on room air 96% on 6L of o2. |
|
On 21-5-21 Spo2: 90% on 10L of o2. |
RESOLVING |
https://nehae-logs.blogspot. |
AT ADMISSION: RR: 22cyc/min Spo2: 96% with 15L of o2 |
|
INCREASE IN SEVERITY: ON 15-5-21 SPO2:88% WITH 15L OF O2 ON 16-5-21 SPO2; 60% OF O2 ON 17-5-21 SPO2: 30% AND WAS INTUBATED. |
|
RESOLVING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
https://prathyushamulukala666. |
AT THE TIME OF ADMISSION: RR: 24 cyc/min Spo2: 88% on room air 95% on 6L of o2. |
14/25 |
At present: Spo2: 90% on room air 93% on 2L of o2. |
RESOLVING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
https://srilekha77.blogspot. |
AT THE TIME OF ADMISSION; RR:24cyc/min Spo2:90% on room air 96% on 6L of o2. |
|
On 19-5-21 Spo2: 95% on 5L of o2. |
RESOLVING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|

Comments
Post a Comment